ABSTRACT
Institutional Goals and Objectives define and inform the curriculum of medical schools. However, an understanding of the curriculum is not complete without understanding what specific educational experiences contribute to the learning and behaviors that the goals and objectives define. The University of Illinois College of Medicine has developed Curriculum Maps to determine the vertical and horizontal threads of learning that build knowledge for students beginning in the basic sciences, as foundational materials, and then build into the clinical curriculum, defining learning from matriculation to graduation. These foundations of knowledge are linked to the Graduation Competencies of the University of Illinois’ Institutional Goals and Objectives and are defined by the educational methods used to present the content and the evaluation methods employed to assess student learning. The process of developing Curriculum Maps, for a complex four-campus medical school, is described along with examples of each step.
INTRODUCTION
In the late 1990’s, the University of Illinois College of Medicine faculty began developing competency-based institutional goals and objectives. These came to be known as the ‘Graduation Competencies.’ Through this work, and developing means to assess the curriculum, it became clear that the relationship of the curricular elements (each required course and clerkship) would need to be linked to the Graduation Competencies in a formal, documented way. Since the professional educators in the College made the argument that developing curriculum maps would aid in developing curricular transparency by providing a system to demonstrate how, where, and when the competencies are met and how competencies are assessed within the curriculum, a discussion of mapping began.
The faculty first explored the advantages and prominence of developing curriculum maps within medicine. The literature revealed that several medical and veterinary schools throughout the world looked to curriculum mapping to manage and provide transparency to their curricula.1-6 Willet and coworkers argues that the integrated curricula found in medical schools are so complex that it is easy to lose sight of the ‘student learning process’ and encourages the use of a mapping system developed within their College for indexing medical topics.1 At the University of Edinburough, UK, faculty developed curriculum maps within the Veterinary College to “…facilitate curriculum review, improve integration and clarity across the curriculum, and provide a transparent method of demonstrating outcomes for quality-assurance purposes.”2 Wong and Roberts worked to map the internal medicine residency curriculum at the University of British Columbia and found their efforts in providing information without duplication resulted in residents satisfied with the curricular presentations and lack of duplication.3 At the University of New South Wales, after developing a new curriculum, the faculty employed curriculum maps as one of several tools to manage the new curriculum.4 Harden at the Centre for Medical Education and Education Development Unit, Dundee, UK, developed a guide published by Association for Medical Education in Europe (AMEE) that encourages medical faculty to develop curriculum maps to “…communicate about the curriculum…”6
Providing leadership and encouraging electronic curricular mapping at the national (United States and Canada) level, the American Association of Medical Colleges (AAMC) has for several years offered a curriculum management tool, CurrMIT7 designed to aid in the management of curricular elements within a medical school, determine curricular gaps and innovations, as well as identify faculty responsible for various elements within a school’s curriculum.8
As early as 1997, the Urbana campus of the University of Illinois College of Medicine began mapping their course and clerkship offerings to the competencies. But not until the Liaison Committee on Medical Education (LCME) review of 2001 did it become clear that the identification of required clinical cases for each clerkship discipline and the identification of required procedures and formal curricular maps would need to be developed to track the curriculum. This was done to assure that the competencies were being met, redundancies were planned, gaps were eliminated and each of the four campuses presented comparable training to students.
Throughout the early 2000’s, the Graduation Competencies were refined by the faculty at the four campuses of the medical school during college-wide retreats. Eventually, they were adopted and revised, most recently in 2007. Simultaneously, the clinical departments adopted cases and procedures for each discipline that students must master in order to pass the corresponding clerkship.
Conceptualizing the Maps
As faculty discussed the information to include in the mapping process, it was clear that linking all required curricular elements to the competencies’ learning objectives was important to evaluate the curriculum. In addition, providing both the educational method employed to present the content and the evaluation method or means with which students were evaluated was necessary. Further, a second set of maps developed to link each of the required curricular elements to the required clinical departments’ cases was made. Both educational methods and evaluation methods were included within these maps. It is important to note that educational methods and evaluation methods* were chosen based on those utilized by the University of Illinois College of Medicine within the Association of American Medical College Curriculum Management Information Tool, CurrMIT7 software database.
Although the literature suggests several commercial products that aid in the mapping process, Microsoft Office Excel was chosen as the spreadsheet of choice because of convenience, familiarity and no additional cost.1, 2, 4, 6, 8-10 Staff and faculty computers are equipped with the Microsoft Office software package and are fully trained on using the software.10
The Process of Mapping
The following is purposefully very detailed, so readers may understand the process employed in developing the curriculum maps for the large and complex curriculum of the University of Illinois College of Medicine. For more information, including additional curricular maps, readers are directed to the web pages of the University of Illinois’ College of Medicine: <a href=”http://www.medicine.uic.edu/” http Also there are two Appendices that provide an example of the output of this process. The process consisted of three major areas: Drawing up the Mapping Form; Collecting Data; and, Constructing the Maps.
1) Drawing up the Mapping Form
In order to collect the data from faculty, templates were designed that would simplify the completion of course/clerkship information. Spreadsheets were designed with multiple pages, one for each Graduation Competency. On every sheet each competency was defined and the corresponding learning objectives were placed along the left hand margin. A legend of Educational Methods and Evaluation Methods was placed at the top of the sheet for ease of use. Templates were developed in a similar fashion for each competency.
2) Collecting Data
Every course and clerkship director was invited to a meeting to submit data by completing template forms. Faculty members were directed to identify objectives from each competency that related to their course, identifying the educational method and the evaluation method employed. For example, basic science course directors were instructed to consider if their course provided fundamental information that supported the attainment of the learning objective; if so they were asked to provide the educational method employed in presenting the materials and the evaluation method used to evaluate the students’ learning. Course directors were encouraged to be inclusive, rather than exclusive, in linking their materials to the learning objectives.
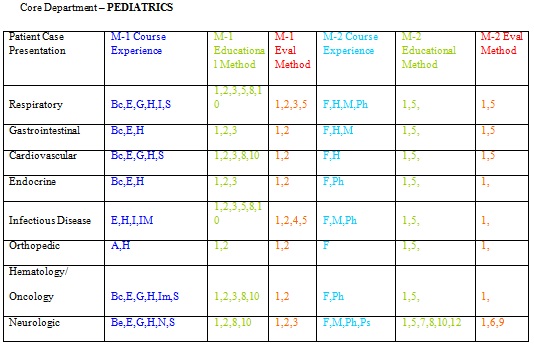
Case Maps
The same process, as described above was followed for Case Maps. Each required curricular offering was mapped to the required cases. This process was repeated at the medical school locations in Chicago, Peoria and Rockford. Appendix 2 Lists the cases by clinical discipline and maps the curriculum to the cases.
CONCLUSION
Curricular Maps were developed for a number of reasons, but the primary one was to provide guides to aid in formal evaluation of the curriculum. The maps were proven to be very useful when matching content to competencies, informing the faculty and students of content flow, and analyzing the curriculum for gaps and redundancies. In addition to that, faculty in the geographically separated Urbana-Peoria-Rockford (UPR) Track found the maps helpful in understanding when particular information was presented in Urbana and how it was evaluated.
Although the LCME site visitors in November 2009 expressed some concern about the comparability of the first year curriculum in Urbana with the first year curriculum in Chicago, the curriculum maps were valuable in demonstrating similarity of the curriculum at different site locations.
One of the challenges in developing the curriculum maps is keeping them current. The maps must change and be updated as the curriculum evolves. This will be an ongoing priority of the faculty and is intended to be built into the curricular evaluation practices of the various curriculum committees.
Employing the Microsoft Office product Excel does have limitations.10 The variety of consumer software products for this specific task of mapping is wide. Features not found in maps built in Excel include flexible reporting tools specific to curricular mapping and other detailed attributes (such as indexing content.) However, the faculty members who utilized the maps feel the instruments currently built are sufficient for basic uses described above.
*The Department of Pediatrics insisted on using specialized evaluation methods that were employed during the Pediatrics Clerkship. They are listed along side the other evaluation methods on the Clerkship Maps.
REFERENCES
- Willett TG, Marshall KC, Broudo M, Clarke M. It’s about TIME: A general-purpose taxonomy of subjects in medical education. Med Educ. 2008; 42(4):432-438.
- Bell CE, Ellaway RH, Rhind SM. Getting started with curriculum mapping in a veterinary degree program. J Vet Med Educ. 2009; 36(1):100-106.
- Wong RY, Roberts JM. Real time curriculum map for internal medicine residency. BMC Med Educ. 2007; 7:42.
- Watson EG, Moloney PJ, Toohey SM, et al. Development of eMed: A comprehensive, modular curriculum-management system. Acad Med. 2007; 82(4):351-360.
- Miller WL. The clinical hand: A curricular map for relationship-centered care. Fam Med. 2004; 36(5):330-335.
- Harden RM. AMEE guide no. 21: Curriculum mapping: A tool for transparent and authentic teaching and learning. Med Teach. 2001; 23(2):123-137.
- Anonymous. Association of American Medical Colleges (AAMC) – Tomorrow’s Doctors. Tomorrow’s Cures.<a href=”http://www.aamc.org/” http. Accessed 4/6/2010.
- Cottrell S, Linger B, Shumway J. Using information contained in the curriculum management information tool (CurrMIT) to capture opportunities for student learning and development. Med Teach. 2004; 26(5):423-427.
- Kathol DD, Geiger ML, Hartig JL. Clinical correlation map. A tool for linking theory and practice. Nurse Educ. 1998; 23(4):31-34.
- Microsoft Office 2010 <a href=”https://partner.microsoft.com/40113273″ https. Accessed 4/7/2010.
Appendix 1

The asterisk on Preceptor Evaluation for Psychiatry refers to a broad definition of Preceptor. In Psychiatry, the Clerkship Director directly observes all students in the clinical setting in addition to teaching didactic sessions, discussing cases, and doing an oral exam.



Core Department-INTERNAL MEDICINE




***image11:center***
***image12:center***
***image13:center***