“Complexity thinking is impossible to define with any precision as it deals not only with change, dynamic change, ever going, but with transformative change. Definitions require stability, the very element complexity neither has nor aspires to have. Instead complexity asks us to see, to deal with a world in continual flux; but a world that does have patterns to it, patterns that bind and structure through their interplay. In short, complexity seeing/thinking asks us to envision our world and events within that world in terms, not of ‘things’ but of process. In so doing, we are moving from a science that studies particles to the new sciences of chaos and complexity that study the interactive relations between and among particles, events, happenings.”1
INTRODUCTION
The purpose of this paper is to disturb the way we think about teaching and learning and to offer a view of health professions education from the perspective of complexity thinking. To discuss complexity and the profound shift it makes with current thinking it is helpful to recall that prior to the 16th century it was believed, in the Western world, that all things on earth and in the heavens were guided by a divine hand.2 Galileo, Newton, Copernicus, Descartes, and Bacon, among others, challenged and changed the status quo. Exploration and the gathering of evidence through experimentation, together with the rise individualism helped give birth to the scientific and industrial revolutions.2 Descartes wrote that everything should be broken down into its smallest component parts in order to understand the whole.2 This has had a profound and lasting effect palpable today in health professions education where mechanistic explanations still prevail and reductionist approaches to curriculum rooted in Cartesian and Newtonian linear causality are common.1-3 This is the dominant paradigm of western science and society. It is how we organize our schools. It is how we teach.
Complexity Thinking
In marked contrast, the vast majority of social and biological events exist in conditions of nonlinear flux and turbulence. Some nonlinear examples include health and illness, the weather, the stock market, the nervous system, ecosystems, social dynamics, teaching and learning to become a health professional. It is difficult, if not impossible, to understand these things by breaking them down into their component parts. Understanding emerges instead from studying the nature of the interactions among the components, the agents.3-10 “Complexity is the result of a rich interaction of simple elements” that only respond to the limited information each of them are presented with. When we look at the behavior of a complex system as a whole, our focus shifts from the individual element in the system to the complex structure of the system. The complexity emerges as a result of the patterns of interaction between the elements.8 Complexity ‘science’ then is the study of nonlinear dynamical interactions among multiple agents in open systems that are far from equilibrium. A brief description of a familiar scenario in health professions education is useful.
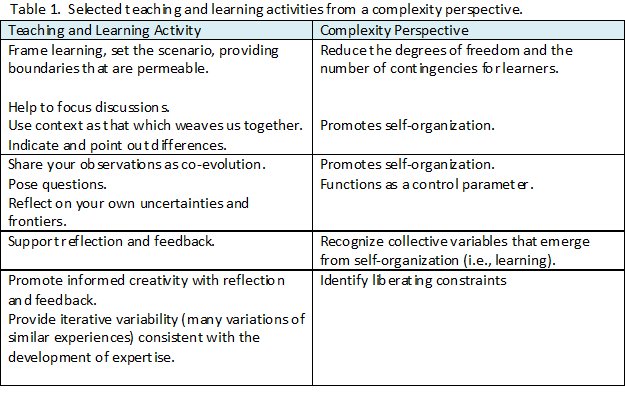
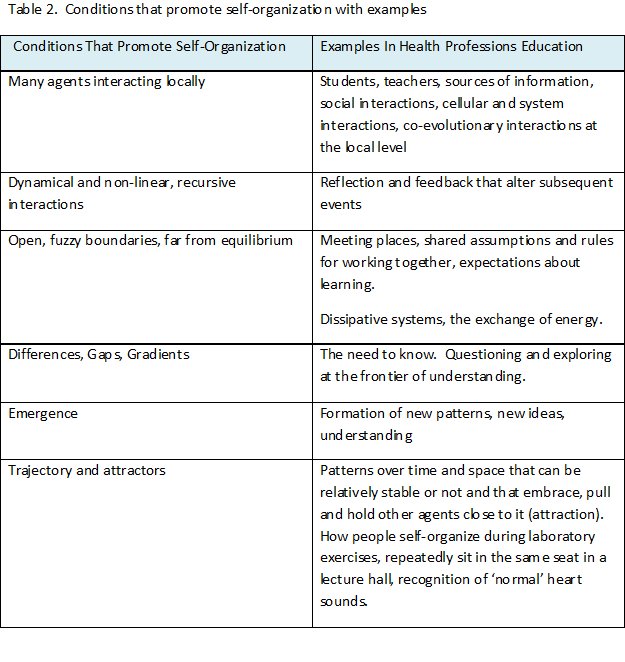
Small-group, discussion-based learning is a good example of a complex system (Table 1).9 There are many people interacting and exchanging information. Each person is also a complex system made up of still more interacting complex systems at different levels. The group meets in a place that is open, people can enter and leave, air, heat and moisture are exchanged. Shared assumptions about the group tasks and expectations about learning provide ill-defined boundaries for the interactions of participants. Each person embodies a different history and experience that structurally enables them to sense and identify gaps in their understanding, “the need to know”. Learners strive to reach the frontiers of their understanding through individual and collective exploration, exchange and collaboration. Doubts and questions function to push the group to the edge of uncertainty where the possibility for self-organization is greatest.11 Self-organization is a process whereby new structures, patterns and properties arise (emerge) in complex systems under particular conditions without being externally imposed on the system.3,8 Learning in complex systems is a self-organized adaptation to changing circumstances.12
As teachers we should understand learning as a dynamical and self-organizing process requiring continuous feedback from multiple diverse interactions. Reflection and feedback promote learning (self-organization). An increased emphasis on formative assessment in health professions education is a healthy development. Traditional education systems refer to knowledge as a noun, as an ‘it’, a commodity that can be conferred, managed and measured. In a dynamical system, knowing is a verb, an emergent interactive process. The complexity perspective describes learning more as a matter of keeping pace with one’s evolving circumstances and less about acquiring and accumulating information.12 Learning requires a constant revision of memories and the capacity for action (understanding).12 Teachers need to use more metaphors. Effective teaching makes use of metaphors for the description of complex events because metaphors both constrain and liberate learners. They attract diverse learners to a collectivity while simultaneously tolerating the ambiguity of creative freedom necessary for connections with the metaphor.
Relationship-Centered Learning
A complex system is sensitive to initial conditions which, although small, can have profound effects on the exchanges between multiple agents leading to self-organization and new patterns. The quality of the exchange between things becomes more important than the things themselves. Teaching and learning are seen as relational and co-evolutionary along a spectrum of “…varying degrees of relative stability, coexisting with, entwined with dramatic, transformative change.”1 There has been an evolution from teacher-centered to learner-centered methods of teaching and learning over the past 40 years. More recently, Suchman has introduced patient-centered care and Gergen has written about reducing the separation between people through what he calls ‘relational being’.13,14 Caring for relationships between people becomes essential in the caring professions. Relationship-centered learning embraces both students and teachers and recognizes and honors the social nature of learning. Conversation and dialogue are seen as a recursive exchange process where understanding emerges in the space between people rather than within them. Learners are simultaneously process, product and producer.12 Relationship-centered teaching values difference and diversity, authentic responsive participation, shared decision-making, collaboration, partnership, and awareness of self and other.14,15 The role of the teacher becomes one of co-evolution rather than the giver of information. Authenticity is expanded beyond the degree of fidelity to the complexities of the workplace to include the quality of the learning relationships that take place between people.
Implications for Teaching
Content expertise may not result in effective teaching just as a great football player may not necessarily be an effective coach. In the complex environment of teaching and learning for the health professions, every moment is a potential teachable moment. Teachers need to be flexible and patient to be comfortable with and skilled at relationship-centered teaching. If interactive learning is to be transformative, there must be ample time for the exchange of differences and time and space for reflection, formative assessment and feedback. The development of expertise and permanent education requires frequent and sustained iterative variability with a collective determination of learning needs for the common good.16
Central to relationship-centered learning is the restoration and strengthening of caring as integral to the process of education of those who must care for others. Seeing the world from the point of view of complexity requires ambiguity and humility “…the striving for certainty, a feature of western intellectual thought since the times of Plato and Aristotle, has come to an end. There is no one right answer to a situation, no formula of best practices to follow in every situation, no assurance that any particular act or practice will yield the results we desire.”1 We are on the cusp of a major shift in thinking with profound implications for what we do as teachers and learners in the 21st century and beyond.
REFERENCES
- Doll Jr, W. E., Trueit, D. (2010) Complexity and the healthcare professions. Journal of Evaluation in Clinical Practice, 16,841-8.
- Doll Jr, W. E. (1993) A post-modern perspective on curriculum. New York: Teachers College press.
- Capra, F. (1996) The web of life: a new scientific understanding of living systems. New York: Anchor books.
- Capra, F. (2002) The hidden connections: integrating the biological, cognitive, and social dimensions of life into a science of sustainability. New York: Doubleday.
- Friedenberg, J. (2009) Dynamical psychology: complexity, self-organization and mind. Litchfield Park, Arizona: ISCE Publishing.
- Holt, T. A. (2004) Complexity for clinicians. Oxford: Radcliffe.
- Sweeney, K., Griffiths, F. (2002) Complexity and health care: an introduction. Abingdon, UK: Radcliffe Medical Press.
- Cilliers, P. (1998) Complexity and postmodernism: understanding complex systems. London: Routledge.
- Mennin, S. (2007) Small-group problem-based learning as a complex adaptive system. Teaching and Teacher Education, 23,303-13.
- Mennin, S. (2010) Complexity and health professions education: a basic glossary. Journal of Evaluation in Clinical Practice, 16,838-40.
- Mennin, S. (2010) Self organization, integration and curriculum in the complex world of medical education. Medical Education, 44,20-30.
- Davis, B., Sumara, D., Luce-Kapler, R. (2008) Engaging minds: changing teaching in complex times. New York: Routlege.
- Suchman, A. L. (2006) A new theoretical foundation for relationship-centered care: Complex responsive processes of relating. J Gen Intern Med 21, S40-S44.
- Gergen, K. J. (2009) Relational being: beyond the self and community. Oxford: Oxford University press.
- Davis, B., Sumara, D. (2006) Complexity and Education: Inquiries into Learning, Teaching, and Research. Mahwah: Lawrence Erlbaum Associates.
- Otero Ribeiro, E. C., Mennin, S. (2010) Continuing Medical Education: Guide supplement 35.2 – Viewpoint. Medical Teacher, 32,172-3.