ABSTRACT
Although animations may intuitively appear more effective than static graphics, evidence for the superiority of computer-based animations is contradictory. This study aimed to investigate whether animations are superior to static graphics as aids to medical students in learning the anatomy and physiology of bladder filling and emptying. We randomized 29 senior medical students into 3 groups: system-paced animations, static graphics, and control. Subjects in the animation and static graphics groups completed a cognitive burden scale and a satisfaction survey immediately after the intervention. All 3 groups completed retention and transfer tests after completion. The difference among the 3 groups was significant for both retention and transfer test scores (F = 10.862, P <.0001 and F = 7.903, P = .002, respectively). Post hoc analysis using Tukey’s HSD revealed no significant difference between the animation and static groups for either retention or transfer. However, both the animation and static intervention groups scored significantly higher than the control group for both retention and transfer (p = .001 and p = 0.003 for animation and p = 0.001 and p = 0.009 for static, respectively). The cognitive load was higher in the animations group but not significantly. Animations did not appear to be superior to static graphics as aids in learning the anatomy and physiology of bladder filling and emptying. Nevertheless, both intervention groups scored better than the control group.
INTRODUCTION
Medical educators are increasingly using animations as part of their teaching and learning activities. However, animations may not always enhance learning, and their creation is time consuming and expensive. Few studies have explored the effectiveness of animations in medical education.1 To learn from static graphics, students must first construct a dynamic mental model. Animations may offer the advantage of illustrating phenomena that might otherwise be difficult to visualize, such as abstract concepts and temporal and spatial relationships.2 Advocates of animations contend that animations offer a more realistic representation of content and thus spare the learner from exerting cognitive effort on the mental construction of a dynamic representation.3 The purpose of this study was to compare the effectiveness of complex, computer-based animations with narrations versus static graphics with narration for the improving transfer of knowledge and student retention.
MATERIALS AND METHODS
Subjects and setting
We recruited 29 third- and fourth-year medical students during their geriatrics clerkship rotation at the University of Miami Miller School of Medicine. We received UMMSM exempted institutional review board approval for this study.
Intervention
Subjects were randomized to 3 groups: animations with narration (n = 10), static graphics with narration (n = 10), and the control group, which received no intervention (n = 9). The time-on-task was approximately 30 minutes. Identical content was used in both interventions and consisted of 8 sets of animations and corresponding static graphics depicting the anatomy and physiology of bladder filling and emptying accompanied by a male voice narration synchronized to the static graphic or to the animation sequence. The students were able to control the onset of each presentation by clicking on the mouse, but otherwise the static graphics and animations were system-paced. The sequence of animations in each set was segmented into a variable number of screens (between 2 and 13) corresponding to the static graphics.
Data Collection
Subjects completed a demographics questionnaire and rated their average knowledge of the anatomy and physiology of bladder filling and emptying on a 5-point Likert scale (ranging from 1, “very little,” to 5, “a great deal of” knowledge). Immediately after the intervention, the students in the intervention groups completed a cognitive burden difficulty-rating Likert scale (ranging from 1, “extremely easy,” to 9, “extremely difficult”) and a satisfaction survey. Then they took a retention test comprising 5 essay-type questions (knowledge) and a transfer test comprising 7 essay-type questions (deeper processing and application). The control group completed the retention and transfer tests without any educational intervention. The intervention groups completed the educational intervention under laboratory conditions, in one sitting and using a desktop computer with a sound card. Two researchers independently scored the subjects’ retention and transfer tests in a blinded fashion. The final score was the average of the two scores.
Data Analysis
Outcome measures were scores on the retention and transfer tests and level of cognitive burden. Descriptive statistics and an ANOVA were used to analyze the results. Cohen D was used to calculate effect sizes.
RESULTS
The 29 medical students in this study were either fourth-year (83%) or third-year (17%). Sixty-one percent were men (21 to 35 years). Subjects rated their knowledge of bladder anatomy as 3.3 in animation, 2.7 in static graphics, and 3.2 in the control group (differences were not significant.)
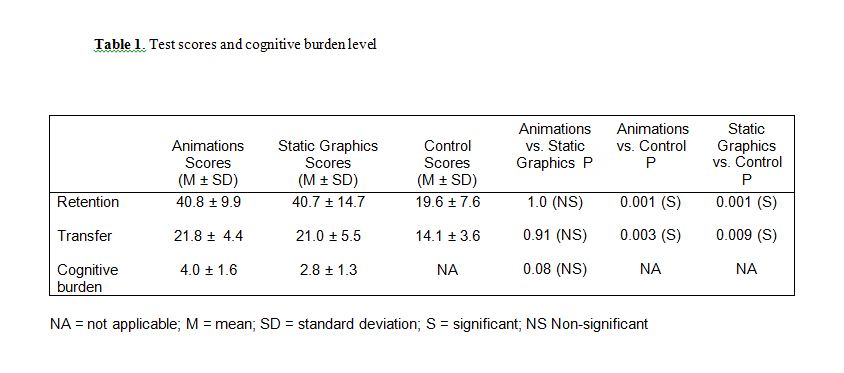
The interrater reliability of the two observers was 0.82 for the retention test and 0.93 for the transfer test. The differences among the 3 groups were statistically significant for both retention and transfer scores (F = 10.862, p < .0001, and F = 7.903, p = .002, respectively). The animation group scored significantly higher than the control group for both retention and transfer (p = .001 and p = .003, respectively) in the post hoc analysis using Tukey’s HSD, with effect sizes of 2.40 and 1.95, respectively. Similarly, the static graphics group also scored significantly higher than the control group for both retention and transfer (p = .001 and = .009, respectively; effect sizes of 1.79 and 1.48, respectively). However, there was no statistical difference between the animation and static graphics groups for either the retention or transfer test scores (Table 1). The mean cognitive burden in the animation group was higher than in the static graphics group (4.0 as compared to 2.8), but the difference did not reach statistical significance (Table 1). Forty percent of the students in the static graphics group expressed boredom about viewing the module as compared to only 20% in the animation group (difference not statistically significant). Twenty percent of the static graphics group, compared to 50% of the animation group, would choose to view the materials again (not statistically significant).
DISCUSSION
We observed significant differences in the retention and transfer test scores between the control group and the interventions. We did not find any significant difference in the scores between the system-paced animation and static graphic groups. We did observe a trend for higher cognitive load and motivation in the animations group.
Our findings are consistent with earlier research on the use of animations in non–health care areas, as well as the findings in a recent naturalistic trial using animations as learning aids for medical students.4,5 Because the learner can control the pace of presentation of static graphics, which may reduce extraneous processing and thus cognitive load, deeper and more relevant cognitive processing and hence better learning may result.2 Animations, on the other hand, may increase extraneous cognitive load and thus impede the selection, organization, and integration of information, which are important for meaningful learning.6 Recent experiments demonstrate that instructional animations depicting human motion tasks are superior to static graphics, but a similar advantage is not seen for abstract, non–movement-based tasks, which is consistent with the results of our study.7
Limitations of the Study
Our findings should be interpreted with caution because of the several limitations to the study. The small sample size may underestimate a true difference between animations and statics in regard to student learning. In addition, we did not assess the baseline knowledge and skills of our subjects in the content area but rather relied on their self-assessments.
CONCLUSION
The effect of animations appears similar to static graphics for student learning as measured by retention and transfer tests, and animations may increase cognitive load. Future larger studies should address the effectiveness and efficiency of learner-paced animation for diverse content areas, with different levels of learners and with different types (and complexity) of animation.
REFERENCES
- Ruiz,J.G., Cook, D.A., Levinson A.J. Computer animations in medical education: a critical literature review. Medical Education 2009;43:838-846.
- Lowe R. Integration of a dynamic visualization during learning. Learning and Instruction 2004;14:257-274.
- Schnotz, W., Lowe, R. External and internal representations in multimedia learning. Learning and Instruction 2003;13:117-223.
- Mayer, R.E., Hegarty, M., Mayer, S., Campbell, J. When static media promote active learning: annotated illustrations versus narrated animations in multimedia instruction. Journal of Experimental Psychology: Applied 2005;11:256-265.
- Tunuguntla, R., Rodriguez, O., Ruiz, J.G., et al. Computer-based animations and static graphics as medical student aids in learning home safety assessment: a randomized controlled trial. Medical Teacher 2008;30:815-817.
- Ploetzner, R., Lowe, R. Dynamic visualizations and learning. Learning and Instruction 2004;14:235-240.
- Ayres, P., Marcus, N., Chan, C., Qian, N. Learning hand manipulative tasks: When instructional animations are superior to equivalent static representations. Computers in Human Behavior 2009;25:348-353.